
Spirometry Tests
A spirometry is a functional test of the lungs. The most important spirometry test is the FVC (Forced Vital Capacity).
Other tests include the CV (Vital Capacity or Slow Vital Capacity) and MVV (Maximum Voluntary Ventilation).
Forced Vital Capacity
The Forced Vital Capacity consists of a forced expiration in the spirometer. The patient either sits or stands. He inspires fully and expires all the air out of the lungs as fast as he can.
The results of the test are compared to the predicted values that are calculated from his age, size, weight, sex and ethnic group.
Two curves are shown after the test: the flow-volume loop and volume-time curve.
The Volume-Time curve explained:

The volume expired in the first second of the FVC test is called FEV1 (Forced Expiratory Volume in the first second) and is a very important parameter in spirometry.
The FEV1% is the FEV1 divided by the VC (Vital Capacity: see next spirometry test on this page) times 100: FEV1%=FEV1/VC X100. Nowadays FEV1/FVC X100 is also accepted as FEV1%.
A healthy patients expires approximately 80% of all the air out of his lungs in the first second during the FVC maneuver.
A patient with an obstruction of the upper airways has a diminished FEV1%.
A FEV1% that is too high is suggestive for a restriction of the pulmonary volume.
After 6 seconds a second parameter is obtained: FEV6. This is more and more used as an alternative for FVC. FEV1/FEV6 can than be used in stead of FEV1/FVC.
The Flow-Volume loop explained:

This is the most important curve in spirometry.
A normal Flow-Volume loop begins on the X-axis (Volume axis): at the
start of the test both flow and volume are equal to zero. Directly
after this starting point the curve rapidly mounts to a peak: Peak
(Expiratory) Flow. If the test is performed correctly, this PEF is
attained within the first 150 milliseconds of the test. The Peak Flow
is a measure for the air expired from the large upper airways
(trachea-bronchi).
After the PEF the curve descends (=the flow diminishes) as more air is expired. After 25% of the total expired volume, the parameter FEF25 is reached.
Halfway the curve (when the patient has expired half of the volume) the FEF50 is reached: Forced Expiratory Flow at 50% of the FVC.
After 75% the parameter FEF75 is reached.
The mean flow between the points FEF25 and FEF 75 is also a very important parameter and is called the FEF2575. This is actually the first parameter that will decline in many respiratory diseases.
It is important to realise that there is no time axis on the flow-volume loop so one can not interpret time intervals. A healthy patient will expire between 70 and 90% of the FVC in the first second of the test. This means that he takes roughly about 5 seconds to expire the last 10 to 30 % of the FVC. The point where the FEV1 is reached is shown on the curve as an illustration.
When the flow reaches zero, the FVC is reached (Force Vital Capacity): the patient has blown out as much air as he can.
After this it is recommended that the patient makes a complete and forced inspiration (to obtain a closed flow-volume loop), but the test can be interpreted without this as well.
The morphology of the
flow-volume loop is very important. To the trained eye the flow-volume
loop tells immediately if the test was well done.
If the flow-volume loop is concave, a bronchial obstruction can be suspected (ie. in the case of COPD).
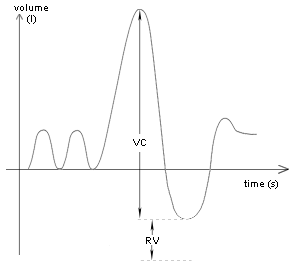
(Slow) Vital Capacity:
This test resembles the FVC. The difference is that the expiration in the spirometer is done slowly. The patient inspires fully and than slowly expires all the air in his lungs (Inspiratory Vital Capacity) or the other way around: the patient expires fully and inspires slowly to a maximum (Expiratory Vital Capacity).
Even if the patient has
expired fully, there is always some air left in the lungs. This is the
Residual Volume. The total Lung Capacity is equal to the (F)VC + the
Residual Volume. The Residual Volume is about 20-25% of the Lung
Capacity.
It is impossible to measure the RV with a spirometer.
More sophisticated methods like the helium dilution test or body
plethysmography are needed to measure the RV.
If the VC is different from the FVC a collapse of the small airways is suspected (if both tests were performed correctly).
Maximum Voluntary Ventilation:
For this test the patient inspires and expires in the spirometer over and over again as fast as he can, during at least 12 seconds.
This is no longer a very common test as it can be dangerous for some people.
Sometimes the MVV is still done in athletes.